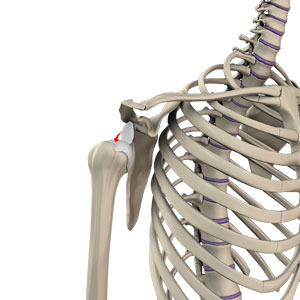
What is Anatomy of the Shoulder?
The shoulder joint is a ball and socket joint. A ball at the top of the upper arm bone (humerus) fits neatly into a socket, called the glenoid, which is part of the shoulder blade (scapula). The glenoid is surrounded by a ring of fibrous cartilage called the labrum for stabilization of the shoulder joint.
What is Shoulder Dislocation?
Sports that involve overhead movements and repeated use of the shoulder at your workplace may lead to sliding of the upper arm bone from the glenoid. The dislocation might be a partial dislocation (subluxation) or a complete dislocation causing pain and shoulder joint instability. The shoulder joint often dislocates in the forward direction (anterior instability), and sometimes in the backward or downward direction.
What are the Symptoms of Shoulder Dislocation?
The most common symptoms of shoulder dislocation include pain and shoulder joint instability. Other symptoms such as swelling, numbness and bruising may also occur. At times, it may cause tears in the ligaments or tendons of the shoulder and nerve damage.
How is Shoulder Dislocation Diagnosed?
Your doctor will examine your shoulder and may order an X-ray to confirm the diagnosis.
How is Shoulder Dislocation Treated?
The condition is treated by a process called closed reduction, which involves placing the ball of the upper arm back into the socket. Following this, the shoulder will be immobilized using a sling for several weeks. Ice may be applied over the area 3-4 times a day. Rehabilitation exercises may be started to restore range of motion, once the pain and swelling decrease.
For more information about our services or to schedule an appointment, call us at / / or click here to request an appointment online. We’ll respond to you as soon as possible.